
Have you ever head the saying “no pain, no gain?” This is one of the most idiotic pieces of advice ever given. Pain is a signal that our body wants us to stop something or that it needs help. I have little doubt that many people have been severely damaged by this so-called piece of wisdom. However, taken to the other extreme, we see people who are so afraid of hard work and exercise that they have become couch potatoes. I believe that many Americans have veered so far off the trail of pain that they have gone to the other extreme. Look around you and what do you see? Fat people everywhere you look. We have an epidemic of obesity in America. Regard the following facts: (From the Center for Disease Control)
- The prevalence of obesity was 36.5% (crude estimate) among U.S. adults during 2011–2014.
- The prevalence of obesity among U.S. youth was 17.0% in 2011–2014.
- From 1999 through 2014, obesity prevalence increased among adults and youth.
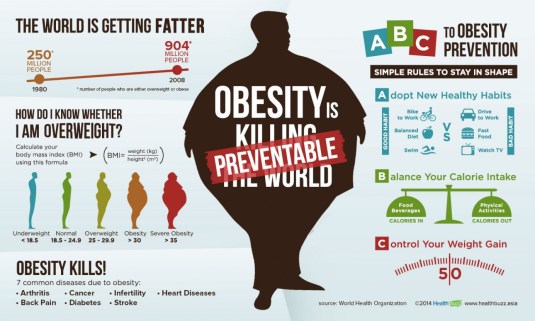
The above data pertain to the frequency of obesity in the USA. Keep in mind that there are many more people who are overweight than there are who are obese. Obesity is defined as: “Excess amount of body fat with a BMI of over 30.” Overweight is defined as: “Having more body weight than is considered normal or healthy for one’s age or build.” If we were to include the amount of people who were both overweight as well as obese, the figures for “fat” people in the USA would skyrocket.
- Almost 3 in 4 men (74 percent) are overweight or obese. — Department of Health and Human Services
Several years ago, I attended a World Future Conference. The former founder and CEO of Medtronic was one of the keynote speakers. His talk was on the topic of rising health care costs. Many people focus on only one or two causes for the escalation of health care costs. However, Earl Bakken presented a pie chart which showed several reasons for the rise. These included:
- Increased cost of technology
- People living longer
- Increased percentage of older people in the population
- Litigation
- Inflation
- Lifestyle choices
Earl noted that all of these issues have had an impact on health costs. You will notice that the last issue in his list included “lifestyle choices.” This category includes such problems as diet, smoking, obesity, drugs, alcoholism, lack of exercise and poor health choices. Contrary to what many people think, this issue was not the major cause of health care cost increases. Nevertheless, the category is one of the factors linked to the increase in health care costs.
Looking only at obesity as a contributor to health care costs, we note the following facts: (From the Health Care Costs of Obesity)
- Obesity is one of the biggest drivers of preventable chronic diseases and healthcare costs in the United States. Currently, estimates for these costs range from $147 billion to nearly $210 billion per year. In addition, obesity is associated with job absenteeism, costing approximately $4.3 billion annually and with lower productivity while at work, costing employers $506 per obese worker per year. As a person’s, BMI increases, so do the number of sick days, medical claims and healthcare costs.
- Obese adults spend 42 percent more on direct healthcare costs than adults who are a healthy weight.
- Per capita healthcare costs for severely or morbidly obese adults (BMI >40) are 81 percent higher than for healthy weight adults. In 2000, around $11 billion was spent on medical expenditures for morbidly obese U.S. adults.
- Moderately obese (BMI between 30 and 35) individuals are more than twice as likely as healthy weight individuals to be prescribed prescription pharmaceuticals to manage medical conditions.
- Costs for patients presenting at emergency rooms with chest pains are 41 percent higher for severely obese patients, 28 percent higher for obese patients and 22 percent higher for overweight patients than for healthy- weight patients.
People who are obese, compared to those with a normal or healthy weight, are at an increased risk for many serious diseases and health conditions, including the following: (From the Center for Disease Control and Prevention)
- All-causes of death (mortality)
- High blood pressure (Hypertension)
- High LDL cholesterol, low HDL cholesterol, or high levels of triglycerides (Dyslipidemia)
- Type 2 diabetes
- Coronary heart disease
- Stroke
- Gallbladder disease
- Osteoarthritis (a breakdown of cartilage and bone within a joint)
- Sleep apnea and breathing problems
- Some cancers (endometrial, breast, colon, kidney, gallbladder, and liver)
- Low quality of life
- Mental illness such as clinical depression, anxiety, and other mental disorders
- Body pain and difficulty with physical functioning
Please notice that the CDC list does not explicitly include hip, knee and back problems. Of course, many people who are not overweight suffer from these problems, but there is considerable evidence that obesity contributes to these problems. People who are obese often lack muscle tissue and ligament flexibility which help support their knees, backs and hips. The less exercise they get, the more the problem is exacerbated. They may go to doctors and chiropractors to get help but the underlying cause of obesity is seldom treated. Finally, surgery is performed when exercise, diet and physical therapy could be more effective treatments. So why do so many people get surgery or pills when there are cheaper and more effective treatments with less side effects?
Let’s go back to what I said in the title of this blog. Laziness and Ignorance.
Laziness and Ignorance:
Every year, it is a well-known fact at health clubs across the country that right after New Year’s Day, the membership will increase dramatically and the parking lot will fill up with new members. This phenomenon will last about 15 weeks after which the new members will slowly drop off and the parking lot will go back to normal. Why do you think this happens? I will give you two reasons:
First: The assumption that they will get instant results. Too many people read the magazines at the grocery store promising “Six Weeks to Abs of Steel” or “Lose 40 lbs. in Eight Weeks.” I would argue that if you can lose 1 lb. in a month, you are doing a great job. As for the abs of steel, first you will need to lose a large amount of body fat and second, it may take you a year of hard dedicated disciplined ab exercises. As someone who does regular ab exercises, they hurt. They are no fun.
 There is a difference between pain and hurt. When I tried to continue my ab exercises after my prostate surgery and then after my hernia surgery, I experienced pain. I wanted to get back into shape too quickly both times. I stopped the exercises and worked on other routines that did not cause pain. Mind you, the ab exercises still hurt and I have been doing them for six years. I am making a big distinction here between pain and hurt. Perhaps, I should say they “burn.” Burn is the athletic euphemism for hurt. Most people don’t like hurt. However, if you expect that you can get in shape without some discomfort, you are destined for life as a couch potato or in a surgery ward.
There is a difference between pain and hurt. When I tried to continue my ab exercises after my prostate surgery and then after my hernia surgery, I experienced pain. I wanted to get back into shape too quickly both times. I stopped the exercises and worked on other routines that did not cause pain. Mind you, the ab exercises still hurt and I have been doing them for six years. I am making a big distinction here between pain and hurt. Perhaps, I should say they “burn.” Burn is the athletic euphemism for hurt. Most people don’t like hurt. However, if you expect that you can get in shape without some discomfort, you are destined for life as a couch potato or in a surgery ward.
Second: People are ignorant when it comes to exercise. How many Americans do you think have ever read a book on exercise? Unless, you are willing to become a student of exercise or trust in an athletic trainer, the knowledge that most people have regarding exercise is insufficient for them to attain the results they seek. Sadly, most medical practitioners are just as ignorant when it comes to the role of exercise and diet in a healthy lifestyle.
How many exercise books do you think make Amazon’s “best seller” list. To determine this, I went to Amazon and pulled up their top 100 best sellers. In the entire list, there was not one book on exercise protocols. There were two books on dieting at number 41 and number 42 in the top 100 list. You could find several books on menus and cooking. It is much easier in the USA to eat, then it is too exercise.
 Americans are enamored with diets and each new diet best seller promises fantastic results in a short amount of time. The Amazon number 1 best seller in the health and exercise category was a book titled “Big Fat Lies.” The author promises you the “truths” that helped her to lose 65 lbs. “without giving up pizza or ice cream.” The author is Kaelin Tuell Poulin and the book has a very high rating in the customer reviews section. Ninety-eight percent of the 235 reviewers gave it a 5-star rating. However, while I often put a great deal of store in ratings, you must be careful about inflated ratings. The one negative rater had this to say about the book: (typos in the review were not changed)
Americans are enamored with diets and each new diet best seller promises fantastic results in a short amount of time. The Amazon number 1 best seller in the health and exercise category was a book titled “Big Fat Lies.” The author promises you the “truths” that helped her to lose 65 lbs. “without giving up pizza or ice cream.” The author is Kaelin Tuell Poulin and the book has a very high rating in the customer reviews section. Ninety-eight percent of the 235 reviewers gave it a 5-star rating. However, while I often put a great deal of store in ratings, you must be careful about inflated ratings. The one negative rater had this to say about the book: (typos in the review were not changed)
“Dont be fooled into purchasing a book that was reviewed by 200 hundred women who never read the book (her followees) I have read the book it is subpar at best and not worth the money. My origional review included picture evidence of her asking for reviews but it was removed because it included her identity i suppose. I hope this one stays up so no one else is fooled into buying this. I give this book 1 star only to post. She is a salesperson and she is a great one at that! but if one person reads this and doesnt feed into the hype it was worth the time and effort to type it.”
I would not call the above review a particularly good piece of criticism. However, the author does alert us to the possibility that the book suffers from a sort of follower worship. Nevertheless, I would risk the small cost of the book if I were looking for a diet program. Consider the following review from one of Kaelin’s “ladyBoss” more ardent followers:
“This program has TWO things that every other weight loss program out there is missing. For ONE Kaelin was heavy once she was 185 pounds herself but with hard work and dedication lost the weight and has kept it off for 5 years.”
This is a great testimonial. I am not sure if “every other weight program is missing” these two factors, but I am sure that dedication and hard work were necessary for Kaelin to keep the weight off for five years. One problem with many exercise and diet programs is that the participant is naive and believes that once they lose the weight, their hard work is over. They may also lack the discipline to continue the work once a certain goal is achieved. Lack of discipline? Laziness? Ignorance? This is a volatile mix. They seem to go together like salt and pepper.
There is one final factor that we must discuss and that studies have shown have a direct bearing on obesity and poor health. This is the factor of poverty. Many studies have shown a direct relationship between income and obesity and between income and exercise. Poor people get less exercise and generally have poorer nutrition. There are several explanations for this. We can posit some possible cause and effect relationships:
- Lack of education leads to obesity
- Poverty leads to high fat diet and poor nutrition
- Lack of education leads to poverty
- Poverty leads to low exercise priorities
You might notice that there is a kind of circularity to the above relationships. Perhaps, if they are circular it does not matter which is cause and which is effect since the result is the same. The outcomes for poor people are poor nutrition, lack of exercise and obesity.
There are some who dispute the above correlations. The claim is made that the relationship between poverty and obesity is not linear but varies by age, gender and ethnicity. It has also been pointed out that rich countries throughout the world have a higher incidence of obesity than poor countries.
“While all segments of the U.S. population are affected by obesity, one of the common myths that exists is that all or virtually all low-income people are far more likely to be obese. In this generalization, two facts commonly are overlooked: (1) the relationship between income and weight can vary by gender, race-ethnicity, or age and (2) disparities by income have been weakening with time, particularly for adults.” — Relationship Between Poverty and Obesity, Food Research and Action Center
However, if we look at obesity from an aggregate point of view and disregard the effects of ethnicity, age and gender, we find the following evidence to show a linkage between poverty and obesity:
“Poverty rates and obesity were reviewed across 3,139 counties in the U.S. In contrast to international trends, people in America who live in the most poverty-dense counties are those most prone to obesity. Counties with poverty rates of >35% have obesity rates 145% greater than wealthy counties.” — Poverty and Obesity by James Levine (2011)
Furthermore, even the Food Research and Action Center admits to the problem that obesity poses for America and state on their site that:
“While all segments of the U.S. population can be affected by poor dietary intake and obesity, low-income and food insecure people are especially vulnerable due to the additional risk factors associated with inadequate resources and under-resourced communities.”
Note the above statement that “poor people” are especially vulnerable. Let me tell you the following story that illustrates some of my admittedly selective experience with this issue of poverty and obesity.
One day, Karen and I went to Scottsdale Arizona to visit and do some shopping. We went to several art galleries and jewelry stores. When it was time for lunch, we found an authentic looking Mexican restaurant and decided to eat outside. We were right in the heart of Scottsdale and many people kept walking by our table. It was fun people watching, but something kept nagging at my mind. I was not sure why, but there was a difference between the average people I was used to seeing and the people I saw in Scottsdale.
Suddenly, I realized what was bothering me. In the hour or so that we were eating, we did not see one obese or even moderately overweight person walk by. All the people that passed by us were healthy and athletic looking. This was my first realization of the connection between wealth and obesity. I don’t know about the rest of the world but ever since then, I have observed that most overweight people I see in America are either poor or middle class. In my opinion, rich people have much lower incidences of obesity in this country.
Aging and Pain:
You will notice that I have not attributed pain to aging. This is not an oversight. Neither is it denial. You can have pain when you are young and you can have pain when you are old. In either case, there is no way you should just accept the pain. Unfortunately, what medical practitioners often diagnose and treat with young people, they are willing to accept with old people. Let me give you another personal example.
 Two years ago, I started developing a pain in my right shoulder. I was not sure where it came from but after several months of it getting worse, I went to see an orthopedic doctor. He asked what if anything I might be doing to aggravate the shoulder. I mentioned that I swim frequently and am aggressive with my laps. His simple answer was “Well then, stop swimming.” I decided to follow his advice and for the next year, I stopped swimming. However, my shoulder pain did not get any better.
Two years ago, I started developing a pain in my right shoulder. I was not sure where it came from but after several months of it getting worse, I went to see an orthopedic doctor. He asked what if anything I might be doing to aggravate the shoulder. I mentioned that I swim frequently and am aggressive with my laps. His simple answer was “Well then, stop swimming.” I decided to follow his advice and for the next year, I stopped swimming. However, my shoulder pain did not get any better.
A year later, I went to see another orthopedic doctor and he could not find anything wrong with my shoulder. He did no MRIs or X-ray’s. I suggested he give me an injection of cortisone, which he did. I had moderate pain relief for about six weeks and then the pain resumed and continued to get worse. At this point, I decided to do some of my own research into shoulder pain. This research was very productive.
I found some very good descriptions of the exact type of pain I was incurring and a few different suggestions on how I could treat the pain without pills or surgery. The best and most positive ideas I found came from a Doctor John M. Kirsch in Wisconsin. Dr. Kirsch put his ideas and supporting evidence for his theory of what causes some types of shoulder pain into a small book titled “Shoulder Pain: The Solution and Prevention.” I have since been following his treatment regimen with good results. My shoulder pain has been decreasing and the range of motion in my right shoulder is improving.
I mentioned earlier that I am 70 years old. I think that there is too often the attitude among people my age and the doctors they see that “pain with aging is inevitable.” If it is inevitable, then we should just “suck it up” and live with it. Sometimes, this might be true. However, the assumption that aging and pain need to go together is a prescription that does not serve any of the elderly very well. I have talked to many older people and I often find the same set of attitudes either on their part or their doctors. It is basically “Well, getting old is a bitch and you just have to live with pain.”
No, you do not have to live with pain!
I have been running 4 or 5 times a week for over 40 years now. During this time, I have had shin sprints, knee pain, hip pain, big toe pain, back pain, Morton’s neuroma, plantar fasciitis, sesamoiditis, corns, calluses and blisters. Each time the pain came, I have gone through the following sequence of activities:
- Awareness of discomfort
- Try to ignore it
- Discomfort moves into the pain stage
- Take over-the-counter meds
- Go to see a doctor
- Pain improved by prescription pills or shots
- Pain returned in a short while
- Do research on other remedies
- Trial and error with other remedies
- Voila, eventually find the right remedy (no surgery and no prescription drugs)
- Pain goes away and does not return
- Sometimes, continuous exercise such as leg stretches and yoga are necessary to keep conditions from returning or getting worse. g., must do calf stretches 3x per week to stop plantar fasciitis from returning.
 Some people are not so lucky. However, I hesitate to call all of my good health “Luck.” There is a saying by Thomas Jefferson that “The harder I work the luckier I get.” I have worked hard to stay in shape. I exercise regularly. I watch what I eat. I try to avoid excesses. No doubt, I have had some luck that goes beyond hard work and discipline. Nevertheless, I believe that hard work and discipline has played a large role in my ability to be healthy and still active at my age.
Some people are not so lucky. However, I hesitate to call all of my good health “Luck.” There is a saying by Thomas Jefferson that “The harder I work the luckier I get.” I have worked hard to stay in shape. I exercise regularly. I watch what I eat. I try to avoid excesses. No doubt, I have had some luck that goes beyond hard work and discipline. Nevertheless, I believe that hard work and discipline has played a large role in my ability to be healthy and still active at my age.
I wish I had a dollar for everyone that has come up to me and said “I wish I could run but I have bad knees.” Many people do have bad knees. But many people do not see a connection between their “bad” knees and their obesity. Their cycle is more like this:
- Overeat
- Gain weight
- Do no exercise
- Get pain someplace
- Do less exercise
- Get more pain
- Go to doctor
- Get knee or hip or some other surgery
- Continue being overweight and doing little or no exercise
- Take pills
The only way the above activities relate to aging is that it takes some time to destroy your body through lack of exercise and poor diet. I guarantee you though, it will happen eventually depending on how much you abuse your body. It may happen when you are young or it may happen when you are old. The longer you wait to do something about it, the more difficult it will be to repair the damage you have done. It seems like my body takes more time to repair itself the older I get.
Finally, you do not have to be rich to have good health. Money will not bring you good health if you abuse your body, overeat, drink too much, smoke too much and avoid exercise. You can pay all the doctors in the world and you will still have bad health if you follow the 10 steps listed above.
Time for Questions:
Do you exercise regularly? Why or why not? Do you have a program to help keep track of your weight? Why or why not? Do you have a weight problem? What do you do about it? How effective have your efforts been? What do you think would help them be more effective?
Life is just beginning.
“My mother was a P.E. teacher, and she was kind of a fanatic about fitness and nutrition growing up, so it was ingrained in me at a young age. As I get older, I’m finding out it’s not about getting all buffed up and looking good. It’s more about staying healthy and flexible.” — Josh Duhamel

 Have you ever heard of a doctor turning anyone down for back surgery, knee surgery or hip surgery by telling them that they are overweight and would be better served by an exercise program or by physical therapy? If so, I can guarantee they are not typical of most medical practitioners. How many doctors look at the major cause of back, knee and hip problems and try to deal with that? Impossible, because doctors do not treat you over a lifetime. You don’t see a doctor until you have a problem and by then it may be too late. Surgery is the fastest solution because exercise, dieting and physical therapy take discipline and time. Doctors do not want to tell you the truth because it is an inconvenient truth but many problems should not be treated by surgery until it is a last resort. Too often, it is the first resort.
Have you ever heard of a doctor turning anyone down for back surgery, knee surgery or hip surgery by telling them that they are overweight and would be better served by an exercise program or by physical therapy? If so, I can guarantee they are not typical of most medical practitioners. How many doctors look at the major cause of back, knee and hip problems and try to deal with that? Impossible, because doctors do not treat you over a lifetime. You don’t see a doctor until you have a problem and by then it may be too late. Surgery is the fastest solution because exercise, dieting and physical therapy take discipline and time. Doctors do not want to tell you the truth because it is an inconvenient truth but many problems should not be treated by surgery until it is a last resort. Too often, it is the first resort. If you have low back pain and see different specialists you will get different tests: rheumatologists will order blood tests, neurologists will order nerve impulse tests, and surgeons will order MRIs and CT scans. But no matter what tests you get, you’ll probably end up with a
If you have low back pain and see different specialists you will get different tests: rheumatologists will order blood tests, neurologists will order nerve impulse tests, and surgeons will order MRIs and CT scans. But no matter what tests you get, you’ll probably end up with a  Recent research has also shown arthroscopic knee surgery works no better than placebo surgery, and when comparing treatments for knee pain, physical therapy was found to be just as effective as surgery, but at significantly reduced cost and risk. And yet another study showed exercise is just as effective as surgery for people with chronic pain in the front part of their knee, known as chronic patellofemoral syndrome (PFPS), which is also frequently treated unnecessarily with arthroscopic surgery.
Recent research has also shown arthroscopic knee surgery works no better than placebo surgery, and when comparing treatments for knee pain, physical therapy was found to be just as effective as surgery, but at significantly reduced cost and risk. And yet another study showed exercise is just as effective as surgery for people with chronic pain in the front part of their knee, known as chronic patellofemoral syndrome (PFPS), which is also frequently treated unnecessarily with arthroscopic surgery.
 So if we assume roughly 326,000,000 (
So if we assume roughly 326,000,000 (
