No matter where you live in American today, you will encounter the problem that there is a physician shortage. It is easy to blame people. We can ask why more people are not interested in becoming doctors. The truth is that America does not suffer from a shortage of people who want to become doctors. It suffers from a healthcare system that systematically limits physician supply, burns out existing doctors, redirects resources toward profit-generating activities, and increasingly treats healthcare as a business rather than a public service.
This issue became more personal for me recently when my wife had three emergency room trips and three overnight stays in the hospital. One for six days, and two for two days each. Despite the fact that no definitive prognosis was found, we could not get an appointment with her pulmonologist for over thirty days after her third emergency visit. My wife was a BA/RN with a master’s degree in public health nursing for over 55 years full time before she retired. I have an undergraduate degree in Health Education. None of our credentials mattered. We were mostly treated like mushrooms. Kept in the dark and fed manure. The reasons we were given “Not enough specialty doctors in our area.”
I have written before about the problems in the American medical system. The problems have only grown worse. Here is a brief summary of where the American Medical System ranks on the five statistics that patients care most about in comparison to other countries.
1. Life Expectancy
This is perhaps the single best measure of whether a healthcare system is helping people live long lives.
- U.S. life expectancy reached about 79 years in 2024.
- That is roughly two years below the OECD average and among the lowest of developed nations.
Why patients should care:
If a nation spends the most on healthcare but its citizens die younger than those in comparable countries, something is wrong with the system.
2. Preventable and Treatable Deaths
These are deaths that should not occur if people receive timely and effective healthcare.
The U.S. has among the highest rates of avoidable deaths among wealthy countries.
Why patients should care:
This measures not whether doctors are talented, but whether the system gets patients the right care at the right time.
This statistic directly relates to physician shortages and delayed access.
3. Access to Primary Care
Primary care physicians are the “front door” to healthcare.
The U.S. has fewer primary care physicians per capita than many peer nations and faces projected shortages of tens of thousands of doctors in coming years.
Why patients should care:
- Longer waits for appointments.
- Delayed diagnosis.
- Greater use of emergency rooms for routine care.
This may be the statistic most directly connected to your physician-shortage article.
4. Infant Mortality
Infant mortality is often considered one of the most sensitive indicators of a nation’s health system.
The United States continues to have a higher infant mortality rate than many other developed countries.
Why patients should care:
If a healthcare system struggles to keep infants alive during their first year of life, it raises questions about access, prenatal care, and healthcare equity.
5. Healthcare Cost
This is where the United States is number one.
- The U.S. spends more per person on healthcare than any other nation.
- Recent estimates place spending at nearly $15,000 per person annually, roughly double many peer countries.
Why patients should care:
Americans are paying luxury-car prices for a healthcare system that often produces middle-of-the-pack—or even worse—results than comparable medical systems in other countries. The following table shows where the USA ranks against the list of OECD countries. The OECD currently consists of thirty-eight member nations most of them high-income democracies.
| Measure | United States |
| Healthcare Spending | Highest |
| Life Expectancy | Near Bottom |
| Preventable Deaths | Near Bottom |
| Primary Care Access | Near Bottom |
| Infant Mortality | Near Bottom |
| Overall Ranking Among Peer Nations | Last |
To verify this data – Go to the Organization for Economic Cooperation and Development site at https://www.oecd.org/en.html
In the blog that follows, I am going to identify some of the major factors that are contributing to the dismal performance of our health care system.
Factor 1: The Doctor Shortage
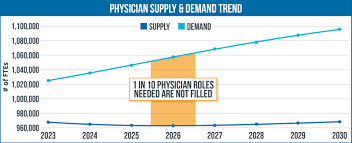
The U.S. is projected to face a shortage of tens of thousands of physicians over the next decade. Rural communities are especially affected, but shortages are increasingly appearing in urban areas as well.
- The Association of American Medical Colleges projects the United States could face a shortage of up to 86,000 physicians by 2036.
- The projected shortage of primary care physicians alone is estimated at 20,200 to 40,400 doctors by 2036.
- Only about 24% of U.S. physicians practice primary care, even though primary care is often the front line for prevention and early diagnosis.
Factor 2: Medical School and Residency Bottlenecks
Most people assume the problem is that too few students want to become doctors.
The reality is more complicated.
Every year thousands of qualified students are rejected from medical schools.
Even after graduation, physicians must complete residency training.
The number of residency positions has not kept pace with population growth because Medicare largely funds residency programs and funding has historically been capped.
Result:
- Fewer physicians enter practice than society needs.
- Existing doctors must see more patients.
- Wait times increase.
Healthcare Outcomes
Patients wait longer for:
- Primary care appointments
- Specialists
- Mental health services
Research consistently shows that delayed care leads to:
- Worse disease outcomes
- More emergency room visits
- Higher mortality rates
Factor 3: Physician Burnout
This may be the most important factor.
- Nearly half of all physicians reported burnout in 2024. One major survey found a burnout rate of 49%.
- Although burnout has improved somewhat, 43.2% of physicians still reported symptoms of burnout in 2024, and 41.9% in 2025.
- Primary care physicians consistently report some of the highest burnout rates in medicine.
Many physicians report spending nearly as much time on:
- Documentation
- Electronic medical records
- Insurance approvals
- Billing requirements
as they spend caring for patients.
Doctors often describe themselves as data-entry clerks with medical degrees.
The Commercialization of the Medical System plays a key role in Doctor Burnout. While it does not directly reduce the number of medical graduates. Instead, it can make physicians less willing to remain in practice.
Think of it as a retention problem.
Doctors often cite:
- Loss of autonomy
- Productivity quotas
- Administrative burden
- Corporate oversight
as reasons for burnout.
When experienced physicians retire early, the effective shortage grows.
Healthcare Outcomes
Burnout contributes to:
- Earlier retirement
- Reduced patient access
- Medical errors
- Lower patient satisfaction
The average patient often experiences this as:
- Rushed appointments
- Less physician attention
- Difficulty obtaining follow-up care
Factor 4: Aging Population
America’s population is getting older.
Older adults consume significantly more healthcare resources.
The Baby Boom generation is moving into years where:
- Cancer rates rise
- Heart disease increases
- Joint replacements become common
- Chronic illnesses multiply
Demand is increasing faster than physician supply.
Healthcare Outcomes
More patients compete for the same physicians.
Wait times lengthen.
Primary care becomes increasingly difficult to access.
Factor 5: Geographic Maldistribution
The United States may not have a pure national shortage as much as a distribution problem.
Doctors tend to locate in:
- Wealthier communities
- Urban areas
- Regions with better reimbursement
Rural America often struggles to attract physicians.
Arizona experiences this challenge in many communities outside Phoenix and Tucson. We live in Arizona City, and the selection of specialists is poor to non-existent here. We are fifty miles from Phoenix and fifty miles from Tucson. Depending on the time of day, it can take two to three hours to get to some areas of Phoenix and two hours to get to some areas of Tucson.
Healthcare Outcomes
Rural patients experience:
- Longer travel times
- Delayed diagnosis
- Higher mortality rates for many conditions

Factor 6: Commercialization of Healthcare
This is where the story becomes particularly interesting.
Many Americans still imagine hospitals as community institutions.
Increasingly they are large corporate enterprises.
Over the past forty years:
- Independent physician practices declined.
- Corporate healthcare systems expanded.
- Investor-owned hospital chains grew.
- Private equity entered healthcare.
Healthcare increasingly became a business sector rather than a public service sector.
Hospital mergers and physician acquisitions frequently increase prices without corresponding improvements in quality.
Factor 7: Hospital Consolidations
- The percentage of physicians employed by or affiliated with hospital systems increased from less than 30% in 2012 to at least 47% in 2024.
- More than three-quarters of U.S. doctors are now employed by health systems or corporations rather than practicing independently.
Thousands of hospitals merged into large regional systems.
Proponents argued consolidation would:
- Reduce costs
- Improve efficiency
- Improve quality
The evidence is mixed.
Many studies suggest consolidation often results in:
- Higher prices
- Greater market power
- Increased administrative costs
Studies reviewed by the Government Accountability Office found that physician and hospital consolidation is generally associated with higher prices and spending, with limited evidence of corresponding quality improvements. Read my blog called, “When Bigger is Not Better.”
Factor 8: Administrative Growth vs Physician Growth
One of the most striking trends is that administrative staffing has grown much faster than physician staffing.
Hospitals employ:
- Compliance officers
- Revenue cycle managers
- Coders
- Contract specialists
- Marketing personnel
- Financial analysts
Many are necessary.
But the growth rate has greatly exceeded physician growth. According to one statistic administrators now outnumber physicians by roughly 10 to 1 in some healthcare systems.
Critics argue the system increasingly rewards administration rather than caregiving.
Healthcare Outcomes
More money flows toward administration.
Less is available for:
- Physician recruitment
- Nursing support
- Patient services

Factor 9: Private Equity and Physician Practices
This is a newer development and one that many people do not know about.
- Approximately 6.5% of physicians worked in private-equity-owned practices in 2024, up from 4.5% in 2022.
While still a minority of practices, the trend is moving rapidly.
Private equity firms increasingly purchase:
- Physician groups
- Emergency departments
- Specialty practices
Their objective is generally to increase profitability and eventually sell the practice.
Critics argue this creates pressure for:
- Higher patient volumes
- More procedures
- Cost cutting
Before concluding Part 1, lets summarize the human cost of the physician shortage in the USA and the attendant commercialism health care in America.
The Human Cost
The physician shortage ultimately affects patients through:
Longer Wait Times
Patients may wait months for specialists.
Reduced Preventive Care
Diseases are detected later.
Overcrowded Emergency Rooms
ERs become substitutes for primary care.
Physician Fatigue
Burned-out physicians are more likely to leave practice.
Health Disparities
Rural and low-income populations suffer most.
Treatment Outcomes
You may die from something that could have been treated with earlier diagnosis.
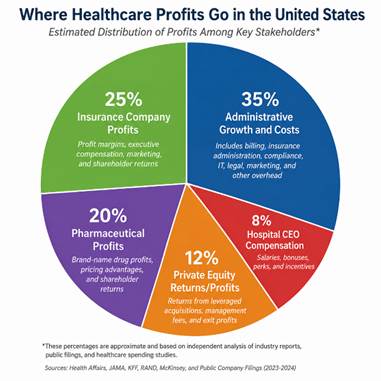
So Where Do the Profits Go:
Consider this paradox. The United States spends nearly twice as much per person on healthcare as many other high-income countries. Yet Americans generally do not live longer, have better access to doctors, or enjoy better health outcomes. If the additional money is not producing better results, where is it going?
After all this discussion about Health Care becoming a business instead of a human service, the obvious question is “Where do the profits go?” There are five main actors in this picture. I would like to call them “villains’ but Metis who is the main author of this piece refuses to let me use this terminology. Hence, here are the five major actors who share in the money pie.
- Hospital CEO Compensation
- Administrative Growth and Costs
- Insurance Company Profits
- Pharmaceutical Profits
- Private Equity Returns/Profits
The easiest way to view the answer to the distribution of profits is to look at a pie chart:
Who Is the Villain? Or is there a Villain?
Whenever Americans discuss healthcare, there is a tendency to look for a villain. Some blame insurance companies. Others blame pharmaceutical firms, hospital executives, private equity investors, politicians, or even doctors themselves. While each of these groups deserves scrutiny, focusing on any single villain misses the larger truth.
The real problem is not one person, one company, or even one industry. The real problem is the system.
Edwards Deming, the quality management expert, often argued that most organizational failures are caused by systems rather than individuals. If Deming were alive today, he would tell us to stop looking for villains and start looking at incentives. Why does the American healthcare system produce higher costs, physician shortages, burnout, and poorer outcomes than many comparable nations despite spending more money than any other country on Earth?
The answer lies in the way the system is structured.
Every major participant in healthcare—hospitals, insurance companies, pharmaceutical firms, physician groups, investors, and government agencies—is responding to incentives that reward revenue growth, complexity, and market power. Over time, these incentives have created a healthcare system that increasingly behaves like a business rather than a public service.
Where does the money go? The largest portion of it disappears into administrative complexity. The United States has built one of the most complicated healthcare financing systems in the world. Hospitals and physician practices employ armies of billers, coders, compliance officers, contract specialists, lawyers, and administrators simply to navigate the rules. Physicians spend countless hours on documentation, insurance approvals, and billing requirements instead of patient care. This complexity contributes directly to physician burnout and rising costs.
Other high-income nations are not perfect, but many have simpler systems, stronger primary care networks, and greater control over prices. As a result, they often achieve comparable or better outcomes while spending far less.
My wife once had a visiting nurse from Sweden come to North Memorial Medical Center where my wife was a nurse manager. Karen was asked to take the visiting nurse and show her around the hospital for the day. She enjoyed the day with the nurse. When Karen came home that evening, she told me about the visit and some of the things that surprised her. This was back in 2005 before Karen retired the first time.
Karen took the nurse to the business center where the people were working on billing and insurance issues. North Memorial was then a 4500 employee hospital and the visiting nurse came from one of comparable size in Sweden. In North Memorial over 200 people were employed in billing and medical coding processes. Karen was shocked to find that in the visiting nurse’s hospital (ALMOST THE SAME SIZE) only three people were employed. Why? Because they had a single payer system with only one place to bill. In the United States, hospital billing can be bewilderingly complex.
A large American hospital may deal with dozens or even hundreds of insurance plans, each with its own reimbursement rules, approval requirements, referral procedures, and appeals processes. What appears to be fifty insurance companies may actually represent hundreds or even thousands of distinct billing arrangements. The result is a healthcare system that requires armies of administrators simply to get paid.
A small rural hospital might have:
- 20–50 major payer contracts
A medium-sized regional hospital might have:
- 50–100 payer contracts
A large urban hospital system may have:
- 100–300 payer contracts
So who is the villain?
The villain is a system that rewards complexity over simplicity, treatment over prevention, administration over caregiving, and financial performance over patient outcomes. Most of the people working within the system are trying to do their jobs well. The problem is that the system often pushes them in the wrong direction.
Until we address those underlying incentives, physician shortages, rising costs, and patient frustration will remain symptoms of a deeper disease. The challenge before us is not to find someone to blame. It is to build a healthcare system that rewards the outcomes patients actually care about: timely access to care, affordable treatment, healthier lives, and better results.
Conclusion
America spends more on healthcare than any nation in history, yet millions struggle to find timely access to a physician. The problem is not a lack of talent or technology. The problem is a system that prioritizes financial performance over system performance. As hospitals consolidate, private equity expands, and administrative complexity grows, physicians increasingly find themselves serving the business of healthcare rather than the practice of medicine. Until we address these systemic issues, doctor shortages will remain a symptom of a deeper disease within American healthcare itself.
If the United States spends more on healthcare than any nation in the world, why do so many patients struggle to find a doctor, wait months for appointments, and feel lost in the system?
If you want more data or resources on any of the subjects I have discussed above, you can find substantial data and references on the following sites. These organizations provide some of the most widely cited and respected data on healthcare spending, physician workforce trends, access to care, and international healthcare outcomes.
1. OECD (Organization for Economic Co-operation and Development)
Best source for:
- International healthcare spending
- Life expectancy
- Physician supply
- Infant mortality
- Cross-country comparisons
General OECD site:
2. Commonwealth Fund
Best source for:
- International healthcare rankings
- “Mirror, Mirror” reports
- Comparisons of U.S. healthcare to other wealthy nations
- Access, equity, and outcomes
3. AAMC (Association of American Medical Colleges)
Best source for:
- Physician shortages
- Residency bottlenecks
- Medical school enrollment
- Workforce projections
Association of American Medical Colleges (AAMC)
4. KFF (formerly Kaiser Family Foundation)
Best source for:
- Healthcare costs
- Insurance statistics
- Medicare and Medicaid
- Hospital consolidation
- Easy-to-understand charts and graphs
KFF (Kaiser Family Foundation)
_____________________________________________________________________________
In Part 2, we will look at what is driving the commercialization of hospitals and why they have become places of profit rather than service. We will also look at some possible antidotes to the commercialization infecting the American Medical System. Some of these solutions will address:
- Expanding residency funding.
- Reducing administrative burden.
- Increasing primary care reimbursement.
- Encouraging independent physician practices.
- Scrutinizing hospital mergers more aggressively.
- Increasing transparency in healthcare pricing.
- Developing rural physician incentives.
- Measuring healthcare success by patient outcomes rather than revenue generation.


Jun 02, 2026 @ 12:09:21
Now that is a complicated system and good luck changing it! I know we have an understaffed medical system here in Canada and like you a lot of our medical personnel tend towards the larger urban centers. However, overall I do think ours works a little better with never a personal care of whether we can afford it.
LikeLiked by 1 person
Jun 02, 2026 @ 12:33:30
Hi Wayne, I think I would take almost any other public medical system like you have or England from what I hear. It is amazing how money can corrupt things so much. My “villain” is the money that corrupts the system and makes these so complext to insure that everyone gets their lb of flesh or shall I say money. Thanks for taking the time to comment. How are thing going with you? John
LikeLike
Jun 02, 2026 @ 12:55:25
Going well and thanks for asking. We are just back home in Nova Scotia from a month visiting friends and family in Western Canada and getting our golf season in swing. I must say I did miss my golf vacation in the the US.
LikeLike
Jun 02, 2026 @ 14:27:33
Glad to hear it Wayne. Hope you golf game is improving 🙂 I could never understand golf. You know the meme so I won’t repeat it. How is economy going up where you live? I have told people down here I hope gas goes to 20 dollars a gallon for regular. They wanted Trump, I will not feel sorry for them. I suppose that sounds cruel on my part, but it is the only thing his followers understand or care about. Gas guzzling pick up trucks that they pay an average of 60 thousand US dollars for and that get poor gas mileage. Boo hoo hoo. 🙂
LikeLike
Jun 02, 2026 @ 17:22:30
Personally I think the world is heading into a very dangerous time and I’m not sad to be 77 with only a few years left to live. I feel bad for my kids and grandkids with the world we are leaving to them and hoping they will maybe not make the same mistakes?
Our economy is stuttering with rising prices bordering on heightened and increasing inflation. But again do we see profits falling?
In my humble opinion we are totally backward in a lot of things– we give tax breaks and incentives to oil companies but not solar or wind development; we give wealthy families incentives to install solar panels or electric cars but no incentives for those less fortunate; we allow development in flood or fire prone areas and then pay them to rebuild when those events happen; and on and on……..
There are some simpler solutions that have been tossed around for decades– a flat tax rate (TBD) for all income(earned or otherwise) with zero deductions; all corporations taxed the same Federally with no provincial/state taxes or incentives to locate there; every dollar earned within our borders by any corporation is taxed equally; the income from every job replaced by robotic means is taxed higher because it is not coming back into the economy.
The idea that we can have ever increasing people, economies and consumption within a closed system is just stupid, it is impossible! We need to transition to a system that is fully functional in which everything consumed is replaced and replenished before it can be consumed again. No matter how we look at it, on a very simple level we need to be able to grow enough of everything we use without diminishing the whole.
Ok, enough of that rant!
LikeLiked by 1 person
Jun 02, 2026 @ 18:40:02
No Wayne, not a rant or tirade. Just a man who feels a lot like I do and perhaps many others. Old age was not supposed to be like this: Climate Change, Covid Epidemic, Trump. Three stikes and we are out. I for one would not come back to this world if you made me a billionaire. Like Jefferson once said to Adams after a 1826 reunion that he felt like a ghost. He realized that he had outlived his time and no longer belonged. I am not comparing myself to Jefferson, but I also feel like I do not belong. So many things do not resonate with me any more. I don’t want to say that this generation is screwed up. I prefer to think they have different values and virtues. Values and virtues which do not fit my lifestyle and which I do not really understand. Anyway, I enjoy connecting with you on a different level and I only wish I had some good advice to give you but I don’t. John
LikeLike
Jun 06, 2026 @ 04:40:06
Thanks John I always enjoy our conversations and it’s good at times to get some frustrations out in a written form.
LikeLike
Jun 03, 2026 @ 11:28:35
Hi, John, I believe this discourse could just as easily be directed at education.
Dennis
LikeLiked by 1 person
Jun 03, 2026 @ 11:58:05
Hi Dennis, Yes I agree. We have a number of “legacy” systems that have not moved with the time or undergone the fundamental system changes that they need. Prisons, Schools, Medical Centers, and of course the Government. IMHO. How are you and Sedna doing? John
LikeLike
Jun 04, 2026 @ 07:44:30
We are doing well. How is Karen doing? Any clarity on root cause of her symptoms?
LikeLike
Jun 04, 2026 @ 08:06:44
Hi Dennis, glad to hear you and Sedna are in good health. Seems we are surrounded these days by bad health. I am still trying to get a referral to another hospital and specialty clinic. They said it would take 72 business hours to get back to me. I did not ask if they included weekends, I just “assumed.” Anyway, Karen is in holding pattern. No diagnois now and no ongoing treatment. She has good days and bad days. In addition, I am now having chest problems and went in for an xray yesterday. Just when I finally got back into a running schedule. I should say life sucks some times, but I won’t because that is just pure narcissism. Trump sucks but that is about the only thing in my world that I am sure SUCKS. The rest is just age, time, nature taking its inevitable toll. Good thing too or can you imagine how many people would be running around on the face of the earth? 🙂 Too many right now as far as I am concerned. Take care Dennis. You will always be a bright spot on the road of my life. John
LikeLike
Jun 11, 2026 @ 07:31:09
Good explanation as to my question as to why we have a shortage of doctors.
Bring back the days a doctor came to your home and sat by the bedside of a sick child. I remember our own family doctor, Dr.Moran. He came in a heartbeat, and I can remember him treating me as a small child when I had strep throat. Those days are gone, and we are left with a system gone awry. 😢
LikeLiked by 1 person
Jun 11, 2026 @ 08:02:41
Thanks for reading Jeanine. Yes, some things were better in the “good old days.” Alas, I think these will never return. One proof that our society and country has gotten too greedy. IMHO.
LikeLike