
This is the first of the ten perspectives I am going to discuss about medical care in the United States in the 21st Century. Before I begin, I have already warned you that if you regard physicians as gods or if you love your MD for saving your life and cannot bear to hear anything wrong about the medical profession, you should probably not read what I am going to say. One of my friends on Facebook sent me this message or caveat:
“I practiced medicine for 30 years. Be careful about generalizing. I got burned out, I cared. I saw the whole person. I’m not unusual. Medicine is hard. You are always looking over your shoulder. Afraid to be sued. We go into this not for money but to help. Really. Believe it.”
I am quite sure that what she says is true. True for some. Not true for others. Is it the majority? I don’t know. But there are a lot for whom the medical system is not working and even more importantly for whom it is dangerous and harmful. Let’s start with some specifics.
After writing and publishing this blog, a good friend of mine reviewed it. He had a very different perspective on things than I present. Together, we are like the Yin and Yang. I see the negative side of things and he sees the positive side of things in the medical profession. It is my belief that we need to see more of the problems with our medical practices and bring them out so that they are more transparent. Nevertheless, I realize that there are thousands of medical people who work hard and try to do their best to help their patients. Thus, I am going to print Fred’s letter to me following my comments. I hope this will “balance” out my negativity somewhat and create a more balanced view of American medical practice in the 21st century. (Thank You Fred for taking the time to send us your thoughts.)
- Number of Needless Surgeries that are Done
There are many people who are enamored with surgery. There are an equal number of doctors who are enamored with surgery. When anyone in the first group goes to anyone in the second group, you can bet that surgery will be the answer to all their problems. Abracadabra! And like magic, their hip pains, knee pains and back pains will go away. The patients are joyous, (unless they die on the operating table like my friend did last summer after going in for a hip replacement). The doctors are joyous since they are thousands of dollars richer and of course the hospitals are also joyous since they too are also thousands of dollars richer.
 Have you ever heard of a doctor turning anyone down for back surgery, knee surgery or hip surgery by telling them that they are overweight and would be better served by an exercise program or by physical therapy? If so, I can guarantee they are not typical of most medical practitioners. How many doctors look at the major cause of back, knee and hip problems and try to deal with that? Impossible, because doctors do not treat you over a lifetime. You don’t see a doctor until you have a problem and by then it may be too late. Surgery is the fastest solution because exercise, dieting and physical therapy take discipline and time. Doctors do not want to tell you the truth because it is an inconvenient truth but many problems should not be treated by surgery until it is a last resort. Too often, it is the first resort.
Have you ever heard of a doctor turning anyone down for back surgery, knee surgery or hip surgery by telling them that they are overweight and would be better served by an exercise program or by physical therapy? If so, I can guarantee they are not typical of most medical practitioners. How many doctors look at the major cause of back, knee and hip problems and try to deal with that? Impossible, because doctors do not treat you over a lifetime. You don’t see a doctor until you have a problem and by then it may be too late. Surgery is the fastest solution because exercise, dieting and physical therapy take discipline and time. Doctors do not want to tell you the truth because it is an inconvenient truth but many problems should not be treated by surgery until it is a last resort. Too often, it is the first resort.
- Data show that 10% to 20% of some common surgeries are done unnecessarily – USA Today – June 20th, 2013
- “I think there’s a higher percentage who are not well trained or not competent to determine when surgery is necessary, Santa says. ‘Then you have a big group who are more businessmen than medical professionals — doctors who look at those gray cases and say, ‘Well, I have enough here to justify surgery, so I’m going to do it.” — USA Today
Here per the study reported by USA Today are the six leading surgeries that often performed and just as often not needed:
- Cardiac Angioplasty, Stents
- Cardiac Pacemakers
Pacemakers are used to correct heartbeat irregularities, but research shows that more than 22 percent of these implants may be unnecessary.
- Spinal Fusion Back Surgery
 If you have low back pain and see different specialists you will get different tests: rheumatologists will order blood tests, neurologists will order nerve impulse tests, and surgeons will order MRIs and CT scans. But no matter what tests you get, you’ll probably end up with a spinal fusion because it’s one of the “more lucrative procedures in medicine,” author Shannon Brownlee says – even though the best success rate for spinal fusions is only 25 percent!
If you have low back pain and see different specialists you will get different tests: rheumatologists will order blood tests, neurologists will order nerve impulse tests, and surgeons will order MRIs and CT scans. But no matter what tests you get, you’ll probably end up with a spinal fusion because it’s one of the “more lucrative procedures in medicine,” author Shannon Brownlee says – even though the best success rate for spinal fusions is only 25 percent!
- Hysterectomy
- Knee and Hip Replacement, and Arthroscopic Knee Surgery
Patients who were informed about joint replacements and alternative treatments had 26 percent fewer hip replacements and 38 percent fewer knee replacements than those who did not. Arthroscopic knee surgery for osteoarthritis is also one of the most unnecessary surgeries performed today, as it works no better than a placebo surgery.
Proof of this is a double-blind placebo-controlled multi-center (including Harvard’s Mass General Hospital) study published in one of the most well-respected medical journals on the planet, the New England Journal of Medicine (NEJM) over 10 years ago.
 Recent research has also shown arthroscopic knee surgery works no better than placebo surgery, and when comparing treatments for knee pain, physical therapy was found to be just as effective as surgery, but at significantly reduced cost and risk. And yet another study showed exercise is just as effective as surgery for people with chronic pain in the front part of their knee, known as chronic patellofemoral syndrome (PFPS), which is also frequently treated unnecessarily with arthroscopic surgery.
Recent research has also shown arthroscopic knee surgery works no better than placebo surgery, and when comparing treatments for knee pain, physical therapy was found to be just as effective as surgery, but at significantly reduced cost and risk. And yet another study showed exercise is just as effective as surgery for people with chronic pain in the front part of their knee, known as chronic patellofemoral syndrome (PFPS), which is also frequently treated unnecessarily with arthroscopic surgery.
According to the World Health Organization, no country is justified in having a cesarean rate greater than 10 percent to 15 percent. The US rate, at nearly 32 percent, is the highest rate ever reported in the US and is higher than in most other developed countries.
The USA Today article went on to talk about many diagnoses that were based on limited medical knowledge and that doctors often lacked the expertise to explore alternative treatment modes. This is an issue of incompetence and it seems to be a major problem in the medical field with many doctors getting their information from their pharmaceutical representatives.
I have not even touched on the issue of malpractice. But I will say a few words about this. No one is perfect. Everyone makes mistakes. Medical treatment and diagnosis is a very difficult process. I will not blame any doctor for an honest error committed with good intentions and not simply out of ignorance or greed. This is one area where I sympathize with the doctors and hospitals more than I do the lawyers. Nevertheless, there are some egregious examples of medical practice and a lawsuit might be the only recourse for such cases.
I use the information from the USA Today article, but none of it surprises me. I have had many friends who have undergone surgery for the situations noted above. I have often tried to counsel them as to other solutions but it is generally a waste of time. I have had two notable successes though and they have both expressed their gratitude to me for sharing my opinions and thoughts with them and preventing them from getting surgery.
- Pills, Pills and more Pills
If life were fair, many doctors would be in jail right alongside of other drug dealers. Doctors do not have the violence associated with illegal drugs because they have a license to prescribe drugs. However, doctors prescribe drugs that are no more needed than heroin or cocaine and at much greater rates than your street drug pusher.
The size of the illicit drug trade (2012 data) in the USA including Marijuana, Heroin, Cocaine and Methamphetamines was estimated to be about 100 billion dollars a year. —- How Big is the U.S. Market for Illegal Drugs? We can assume that street dealers and drug pushers are responsible for most of these drugs. So how much do doctors push?
If we look at the following fact, we can extrapolate from it the total amount of prescription drugs sold each year in the USA.
“In 2013, per capita spending on prescription drugs was $858 compared with an average of $400 for 19 other industrialized nations. In the United States, prescription medications now comprise an estimated 17% of overall personal health care services. — The High Cost of Prescription Drugs in the United States (2016).
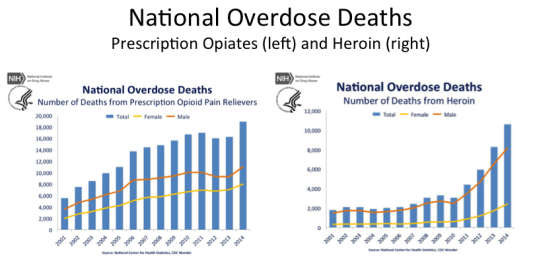 So if we assume roughly 326,000,000 (USA Population in 2016) people and we multiply that by $858 dollars per capita, the total amount should equal the total amount spent on prescription drugs. This amount equals = $279,708,000,000. This is almost three times what is being spent on illegal drugs. I am not even going to talk about caffeine, alcohol, nicotine, and other “legal” drugs. Given that doctors love to prescribe pills and many patients love to take them, is there any wonder that we have or are currently experiencing an opioid epidemic in the US.
So if we assume roughly 326,000,000 (USA Population in 2016) people and we multiply that by $858 dollars per capita, the total amount should equal the total amount spent on prescription drugs. This amount equals = $279,708,000,000. This is almost three times what is being spent on illegal drugs. I am not even going to talk about caffeine, alcohol, nicotine, and other “legal” drugs. Given that doctors love to prescribe pills and many patients love to take them, is there any wonder that we have or are currently experiencing an opioid epidemic in the US.
“Americans are in more pain than any other population around the world. At least, that’s the conclusion that can be drawn from one startling number from recent years: Approximately 80 percent of the global opioid supply is consumed in the United States…. The 300 million pain prescriptions equal a $24 billion market.” — Americans consume vast majority of the world’s opioids (2016).
I say again that if life were fair, many doctors would be called drug pushers or DP’s rather than MD.’s They would also be in jail. Who should be responsible for the opiate epidemic if not doctors. When and where do they stand their ground. Even if people are stupid or lazy enough to want surgeries to cure problems of obesity and diet or if they want pain killers to mask the problems from their obesity and lack of exercise, who is the expert here? Do parents give their children everything they ask for? You go to an expert on medicine to get help and not to have them take advantage of you for their own benefit or pander to you because they are afraid to tell you the inconvenient truth. What is this inconvenient truth? I will talk more about this truth later in this series but to be quite direct and blunt it is this:
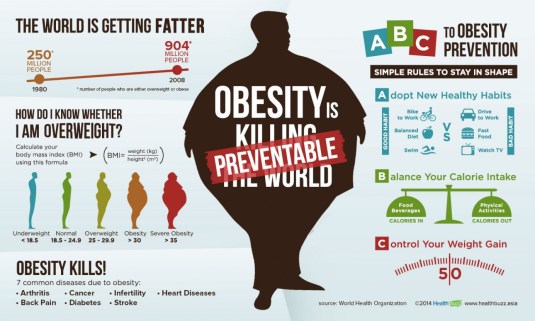
“British businesswoman and columnist Katie Hopkins has a controversial view on the obesity epidemic: that the solution is simply to eat less and exercise more — and that fat people have no one to blame for their weight issues but themselves.” — I gained 43 pounds to prove obese people are lazy
I had a friend that I used to ride motorcycles with. He died in a motorcycle crash a few years back. He was a great guy. He always had a smile and something nice to say to someone. His name was Gary. He was also obese and exercised little. He had chicken legs and bad knees. Well, what would you expect if you weighed 100 lbs. more than you should and you let your leg muscles go to hell. Of course, he went in to see his doctor with knee pains. The doctor was more than happy to suggest Gary should lose some weight but in the meantime, he would schedule the surgery for knee replacement. To my mind, this is criminal, irresponsible and ignorant behavior on the part of his doctor. Gary got the surgery. Never lost much weight and died not too long after from other causes.
Doctors pushing pills, pushing surgery. It is like the Yin-Yang of American medical practice. Throw into the mix a lot of lazy people who do not exercise or take care of themselves and you have a health care system spending tons of money on acute care when preventive care would be a much more sensible solution.
- Me Doctor, Me Busy. Who are You?
Some of you might remember the skit on Saturday Night Live with Martin Short playing a doctor. When asked what his badge that said MD meant, he would reply somewhat superciliously “Me Doctor, You Patient.” When I was working as a consultant to some hospitals, it was not uncommon to hear nurses complain that doctors were like gods whose every word should be obeyed. They seldom came to team meetings because “their time was too valuable.”
I will stay away from the subject of how much money doctors rake in since they often ascribe their high incomes to the length of time it takes to finish medical school and all of the attendant costs. This sounds like a reasonable explanation but an alternative theory might mention the strangle hold that the AMA had on medical admissions and the role that restricting the supply of doctors has had on the cost of their services. The law of supply and demand says that if you have fewer doctors, the cost per care will be higher. For years, the AMA did all they could to help keep the supply of doctors down.
- But the entities that will be most injurious to the nation’s health are not so much in the evil-mongers’ group but the first group, including the American Medical Association–a doctors’ cartel that has controlled the medical labor market in the U.S. like its personal fiefdom for a century. — The Evil-Mongering Of The American Medical Association (2012)
So, doctors come to regard themselves as the elite who know more than you do and who must be smarter than you since they make a great deal more money than most of their patients. Doctors used to do house calls many years ago; back then, a doctor might have known something about your family and you personally. My wife Karen told me the following story about her family doctor. It generated the following conversation:
Karen —
“When I was married, and raising four children, my ex-husband Ron and I became good friends with a local White Bear doctor. He became a family friend as well as our family doctor. We knew him for over thirty years and he knew me and my family personally and really cared about us.”
John —
“Okay, so now you have been seeing a doctor in Frederic for about seven years. How much does she know about you personally or really care about you?”
Karen —
“I think she really cares about me.”
John —
“But how much does she know about you personally. Your goals. Your dreams. What you did this past winter?”
Karen —
“Well, at first, she used to take more time to talk to me but the past few years she has seemed much busier and anxious to keep our meetings short. I suppose the clinic has a quota for how much time she can spend with a patient.”
Again, there are numerous anecdotes and articles describing the lack of time doctors have to spend today with patients. Here is an excerpt from one:
“Joan Eisenstodt didn’t have a stopwatch when she went to see an ear, nose and throat specialist recently, but she is certain the physician was not in the exam room with her for more than three or four minutes.
‘He looked up my nose, said it was inflamed, told me to see the nurse for a prescription and was gone,’ said the 66-year-old Washington, D.C., consultant, who was suffering from an acute sinus infection.
When she started protesting the doctor’s choice of medication, “He just cut me off totally,” she said. “I’ve never been in and out from a visit faster.” — You’re on the clock. Doctors rush patients out the door (2014)
I can guarantee you that if your doctor only takes a few minutes with you, once or twice per year, there is not much they can know about you personally regardless of how caring and concerned they are. You might ask “well, why is this important.” Here is the reason stated very well I think in Wikipedia:
“The quality of the patient–physician relationship is important to both parties. The better the relationship in terms of mutual respect, knowledge, trust, shared values and perspectives about disease and life, and time available, the better will be the amount and quality of information about the patient’s disease transferred in both directions, enhancing accuracy of diagnosis and increasing the patient’s knowledge about the disease. Where such a relationship is poor the physician’s ability to make a full assessment is compromised and the patient is more likely to distrust the diagnosis and proposed treatment, causing decreased compliance to actually follow the medical advice.” — Wikipedia
Conclusions:
I promised some solutions to each truth that I am telling you. Here are some that might help you to deal with this first truth.
- Get a second opinion for any surgery.
- Use the Internet to search for alternative treatment modes. Get advice if you are not Internet savvy. Remember, there are many opinions and not all are right.
- Exercise and have a health care plan. Follow it.
- Don’t take any pills unless you must. Try to unwean or get off them as soon as possible.
- Beware side effects from pills. Every pill has a side effect. Make sure you are aware of any that might affect you and be cognizant of any changes in your life while taking these pills.
- Take a friend with you whenever you go in for an appointment or treatment. Talk to your friends to get their insights and opinions.
- Don’t assume your doctor is God and knows what is best for you. Be a skeptic but be realistic. Modern medicine is better than sorcery but not always much better.
- Don’t assume that your doctor is your friend or has your best interests at heart. They might not have enough time to care.
Fred’s letter to me:
I read your blog on medical practice and it was indeed thought provoking.
I’ve had good results with doctors over my lifetime. Not always perfect but usually satisfactory and in some cases, it was excellent.
Medical care is a process and requires the same attention as any process. It seems especially complex today because of how rapidly technology and all the stakeholder’s needs and expectations are changing.
Overall, it’s greatly improved in its capabilities. My main concern for medicine is the same as I’ve had for years in business. My business life became more and more controlled by the bean counters and the lawyers. The same is true of medicine. Blaming doctors is blaming people, which is always a red flag to me as one who has a bad habit of judging others without knowing them. Like the driver for quality improvement, expectations always move to higher and higher expectations. And based on what I’ve heard from friends over my life, expectations are often unrealistic.
A friend recently died. He was an old school, oil field production engineer and didn’t trust any of his doctors. He’d get pissed at one and then begin to “doctor hop”; never telling one what the other had done or prescribed. I questioned him many times, always inquiring why he’d not share his history. His reply: “I ain’t telling them anything. They make good money and are supposed to tell me what’s wrong.”
I see the process much as we viewed our manufacturing and service processes ..with customers, suppliers, inputs and outputs being carefully considered. A critical output is the result when your illness is diagnosed and this is too often a major problem source. My friend tends to expect this to be an exact outcome but in reality it isn’t. It’s only a statistical prediction that too many older doctors failed to point out to naive, uneducated patients.
In recent years, our doctors point out the statistics and involve us in the decisions for corrective action. My wife’s breast cancer surgery was a good example. Years ago, the doctor would have made the decision for which surgery, mastectomy or lumpectomy. Sandra made the decision armed with various study statistics and discussion with the Doctor. The Internet was a source for me to verify the statistics but that isn’t easy because there are often many studies,
The surgeries are complex and the statistics often work out for the worst. Records on lawsuits and doctor reviews are more readily available today. I recall a bad experience with my dad years ago. Our family doctor became a friend from making many house calls as 3 kids were raised. Dad was a merchant seaman and would provide Porte Rico rum for our good doctor. They were the best of buddies and talked about the old days during visits. Dad visited him yearly but when dad’s tobacco tarred lungs became late stage cancerous it was too late. Doctor “Tom” as an individual practitioner didn’t have the computer technology that red flags today’s doctors. Doctor Tom was as heartbroken as my dad. He and his wife nurse apologized that they’d not x rayed dad 6 months earlier. We probably could have sued but dad would never have agreed to such.
The body of knowledge has expanded too much for any one doctor to master it all, so now we have multiple knowledge based “Specialists” having to deal with the directives from medical organization bean counters and their lawyers.
I consider our medical providers to be leading edge. They seem to focus on continuously improving to meet customer expectations. I’m hoping, but doubt the doctors and staff will be given additional support. They track customer satisfaction inputs so I should be more confident.
I can email any of my doctors and I can access historical results. I especially like being able to take a picture of a physical observation and sent it in. A couple of years ago, I tore a muscle on the back of my leg and a huge blue area surfaced overnight. It scared the heck out of me. I emailed a picture and he emailed back telling me what it probably was, how to treat it and to see a doctor if it didn’t heal. My expectations are now at an even higher level which puts more load on the doctor. He not only has to live up to corporate standards on office visits but he must respond to patient emails. Just yesterday I received a corporate email announcing that they have decided to do “Face Time” appointments for $25!
Overall, I have concerns for the profession but I think problems are “process” related. To think otherwise would go against what I’ve believed for a long time.
Fred
Time for Questions:
How satisfied are you with your medical care? Why or why not? Have you ever had a loved one die? How were they treated by the medical profession? What do you think could be done to improve medical care for you and your family? What would you like to change in the American medical care system?
Life is just beginning.
“We have really good data that show when you take patients and you really inform them about their choices, patients make more frugal choices. They pick more efficient choices than the health care system does.” — Donald Berwick

 I am not a very sentimental person nor am I one to cling to the past. I decided I would move on with my life. I threw myself into my job and time went by. I had almost forgotten about Leandra when I saw the ad. It was from the Resurrection Android Company. It was the same company that I had purchased my android valet Sam from. Actually, Sam was much more than just a valet. Sam was a third-generation android with some independent powers of decision making. He could decide what to cook each day and he also decided what I should wear for work. He did cleaning, mending and many light repairs around the house. I had bought Sam shortly after Leandra and I were married. Leandra had mentioned that it would be nice to have some help with housekeeping and all. That way she would have more time to spend with me.
I am not a very sentimental person nor am I one to cling to the past. I decided I would move on with my life. I threw myself into my job and time went by. I had almost forgotten about Leandra when I saw the ad. It was from the Resurrection Android Company. It was the same company that I had purchased my android valet Sam from. Actually, Sam was much more than just a valet. Sam was a third-generation android with some independent powers of decision making. He could decide what to cook each day and he also decided what I should wear for work. He did cleaning, mending and many light repairs around the house. I had bought Sam shortly after Leandra and I were married. Leandra had mentioned that it would be nice to have some help with housekeeping and all. That way she would have more time to spend with me. Androids of course are not human and they have no empathy or ability to show any emotions. Sam was logical and could be persuasive but he could not show love or compassion. In the ten years since I had purchased Sam, android technology had advanced considerably. Looking at the ad from the company, it appeared that they were now on a 15th generation android that had affective as well as cognitive abilities. The ad claimed that the new android could help replace a loved one both emotionally and physically. By integrating DNA characteristics using a technique called “Assisted human reproduction”, they could capture the exact characteristics of a loved one. All they would need would be some trace or remnant of the deceased or former loved one’s DNA.
Androids of course are not human and they have no empathy or ability to show any emotions. Sam was logical and could be persuasive but he could not show love or compassion. In the ten years since I had purchased Sam, android technology had advanced considerably. Looking at the ad from the company, it appeared that they were now on a 15th generation android that had affective as well as cognitive abilities. The ad claimed that the new android could help replace a loved one both emotionally and physically. By integrating DNA characteristics using a technique called “Assisted human reproduction”, they could capture the exact characteristics of a loved one. All they would need would be some trace or remnant of the deceased or former loved one’s DNA. That was when the idea occurred to me. I called the customer service line and asked to speak to a representative. I asked her whether it would be possible for me to create a new wife in the exact image of my former wife Leandra. They assured me it was. It would take about six months for the bio-engineering to integrate the mechanical aspects of the droid with the alleles and DNA strands that they could map from a sample of Leandra’s DNA. When the process was completed, I would have an exact physical, mental and emotional copy of Leandra. Even better, she could continue to be programmed and become an even better Leandra. The old Leandra was somewhat boring in bed. The new Leandra could become a wild and wanton partner if that is what I desired.
That was when the idea occurred to me. I called the customer service line and asked to speak to a representative. I asked her whether it would be possible for me to create a new wife in the exact image of my former wife Leandra. They assured me it was. It would take about six months for the bio-engineering to integrate the mechanical aspects of the droid with the alleles and DNA strands that they could map from a sample of Leandra’s DNA. When the process was completed, I would have an exact physical, mental and emotional copy of Leandra. Even better, she could continue to be programmed and become an even better Leandra. The old Leandra was somewhat boring in bed. The new Leandra could become a wild and wanton partner if that is what I desired. It did not take long to assemble the new Leandra. I put the lower torso, upper torso and head together in less time than it takes to make a milk shake. She was perfect. She looked just like my old Leandra. When I turned her on, she greeted me and asked, “What will my name be.” I replied “You are Leandra. You are the perfect wife. You will love and obey me always.”
It did not take long to assemble the new Leandra. I put the lower torso, upper torso and head together in less time than it takes to make a milk shake. She was perfect. She looked just like my old Leandra. When I turned her on, she greeted me and asked, “What will my name be.” I replied “You are Leandra. You are the perfect wife. You will love and obey me always.” I came home one day from work and Leandra did not greet me at the door. I thought maybe her battery had discharged or that Sam had forgotten to recharge her. I had left strict instructions for Sam to recharge Leandra every day. But, where was Sam? I did not hear him fixing dinner in the kitchen. I went into the kitchen but Sam was not there. Suddenly, I noticed a note on the table. I picked it up. It was from Leandra. She had written: “Gone with Sam, don’t love you anymore. Bye.”
I came home one day from work and Leandra did not greet me at the door. I thought maybe her battery had discharged or that Sam had forgotten to recharge her. I had left strict instructions for Sam to recharge Leandra every day. But, where was Sam? I did not hear him fixing dinner in the kitchen. I went into the kitchen but Sam was not there. Suddenly, I noticed a note on the table. I picked it up. It was from Leandra. She had written: “Gone with Sam, don’t love you anymore. Bye.”

 All of my family and relatives attended both of these productions. We are a very close knit family and we wanted to show support for my sister. Six years ago, some of my family had wanted to go to the tattoo parlor with me when I had my first tat. I decided to go by myself. It was something that I felt that I had to do alone. The problem or conundrum I faced was what kind of a tattoo should I get and what part of my anatomy should I get it on? I remember that I had lots of advice on the matter. My father, mother, sister, grandmother, grandfather, aunts, uncles, nieces, nephews and friends all had tons of ideas and suggestions related to both questions.
All of my family and relatives attended both of these productions. We are a very close knit family and we wanted to show support for my sister. Six years ago, some of my family had wanted to go to the tattoo parlor with me when I had my first tat. I decided to go by myself. It was something that I felt that I had to do alone. The problem or conundrum I faced was what kind of a tattoo should I get and what part of my anatomy should I get it on? I remember that I had lots of advice on the matter. My father, mother, sister, grandmother, grandfather, aunts, uncles, nieces, nephews and friends all had tons of ideas and suggestions related to both questions. I received numerous suggestions on the best place to have a tattoo. Some suggested it be placed where I could easily cover it up when I did not want it be seen. Others suggested that it be someplace more visible. Some said to get it on my shoulder or thigh where I could show it off during the warmer summer months while wearing shorts or a tank top. Places like my lower arms would be visible more often but also more difficult to conceal. Another dilemma, where to get my tattoo placed?
I received numerous suggestions on the best place to have a tattoo. Some suggested it be placed where I could easily cover it up when I did not want it be seen. Others suggested that it be someplace more visible. Some said to get it on my shoulder or thigh where I could show it off during the warmer summer months while wearing shorts or a tank top. Places like my lower arms would be visible more often but also more difficult to conceal. Another dilemma, where to get my tattoo placed? With the looming appointment for my tattoo, I had even more pressure now to decide “What was I going to get? What would my first tattoo be? How do I find something truly unique?” I thought about it all week. Every TV show I watched, everything I read, more advice and suggestions from well-meaning advisors but nothing really excited me. I went on the Internet. I went to the library. I looked at tattoo magazines with numerous women and men who had tats. I must have looked at a thousand pictures of different tattoos but still nothing resonated. I did not want any of the tats that I had seen.
With the looming appointment for my tattoo, I had even more pressure now to decide “What was I going to get? What would my first tattoo be? How do I find something truly unique?” I thought about it all week. Every TV show I watched, everything I read, more advice and suggestions from well-meaning advisors but nothing really excited me. I went on the Internet. I went to the library. I looked at tattoo magazines with numerous women and men who had tats. I must have looked at a thousand pictures of different tattoos but still nothing resonated. I did not want any of the tats that I had seen.
 The point of this story is that if we had not been siting vigil at my sister’s deathbed, we would not have been able to prevent a premature death. This is merely one example of the value of an “advocate” when you must go to a hospital. I am sure everyone reading this blog has at least one example that highlights how important it is to have someone as an advocate when you are in the hospital.
The point of this story is that if we had not been siting vigil at my sister’s deathbed, we would not have been able to prevent a premature death. This is merely one example of the value of an “advocate” when you must go to a hospital. I am sure everyone reading this blog has at least one example that highlights how important it is to have someone as an advocate when you are in the hospital. An alarm might go off in an intensive care room but not be noticed for quite some time. I have personally observed many times when a patient needed to call someone for assistance but no one came. Unable to get out of bed, a patient may have to wait a long time before someone is finally able to help them. In many cases, an advocate in the room can help a patient with minor personal needs. If more severe needs exist, the advocate can be of assistance if finding someone to help and making sure that the patient needs are not overlooked or even forgotten.
An alarm might go off in an intensive care room but not be noticed for quite some time. I have personally observed many times when a patient needed to call someone for assistance but no one came. Unable to get out of bed, a patient may have to wait a long time before someone is finally able to help them. In many cases, an advocate in the room can help a patient with minor personal needs. If more severe needs exist, the advocate can be of assistance if finding someone to help and making sure that the patient needs are not overlooked or even forgotten. Another function an advocate can provide is to stand up for the patient when needed. Most of the time when we are feeling sick or hurting, we are in no position to stand up for what we need or want. In such instances, a patient only wants the pain to go away. Hospitals and health care providers often have needs that transcend the needs of the patient. The patient that must play second fiddle to a variety of administrative and financial procedures. Another example might clarify this.
Another function an advocate can provide is to stand up for the patient when needed. Most of the time when we are feeling sick or hurting, we are in no position to stand up for what we need or want. In such instances, a patient only wants the pain to go away. Hospitals and health care providers often have needs that transcend the needs of the patient. The patient that must play second fiddle to a variety of administrative and financial procedures. Another example might clarify this.

 Being overly competitive might be a good formula in exercise programs where you attempt to outdo other participants, but this can be another recipe for disaster when it comes to Yoga. Each participant in Yoga needs to pay attention only to their own body; not to the other participants or even the instructor. If the instructor has his/her legs at a 180 degree angle to their torso and you can only make 30 degrees, you are best advised not try to imitate your instructor or other participants. A good instructor will repeatedly advise you to only go as far as you can with any Yoga posture. Pushing the envelope may lead to torn muscles or dislocated joints.
Being overly competitive might be a good formula in exercise programs where you attempt to outdo other participants, but this can be another recipe for disaster when it comes to Yoga. Each participant in Yoga needs to pay attention only to their own body; not to the other participants or even the instructor. If the instructor has his/her legs at a 180 degree angle to their torso and you can only make 30 degrees, you are best advised not try to imitate your instructor or other participants. A good instructor will repeatedly advise you to only go as far as you can with any Yoga posture. Pushing the envelope may lead to torn muscles or dislocated joints. Start doing Yoga once or twice a week. You can get a Yoga mat, strap, blocks and some used Yoga DVD’s for less than $30 dollars. With some Yoga tapes and a DVD player, you will be able to do Yoga in the privacy of your home and as often as you want. I have found Rodney Yee, Patricia Walden and Susan Deason to be great instructors. Gaiam Yoga tapes can often be found in Goodwill or other thrift stores for a few dollars each. On frigid days, it is a real pleasure not to have to get dressed and go to a gym. It is also great to have an instructor on DVD that I do not have to keep paying weekly fees to.
Start doing Yoga once or twice a week. You can get a Yoga mat, strap, blocks and some used Yoga DVD’s for less than $30 dollars. With some Yoga tapes and a DVD player, you will be able to do Yoga in the privacy of your home and as often as you want. I have found Rodney Yee, Patricia Walden and Susan Deason to be great instructors. Gaiam Yoga tapes can often be found in Goodwill or other thrift stores for a few dollars each. On frigid days, it is a real pleasure not to have to get dressed and go to a gym. It is also great to have an instructor on DVD that I do not have to keep paying weekly fees to.









 Are you still wondering why drug costs are so high? Did you really think it was all research and development costs? The three major factors are: Profits, lobbying and Marketing. How much do you think these all add to the costs of your prescription drugs?
Are you still wondering why drug costs are so high? Did you really think it was all research and development costs? The three major factors are: Profits, lobbying and Marketing. How much do you think these all add to the costs of your prescription drugs?
 There are many other egregious practices that go on in Big Pharma and which are beyond the scope of this blog. My point in writing this was first to help alert you to the hypocrisy of the so-called drug wars and second to bring to your attention the inordinate amount of effort and money that Big Pharma spends in trying to get you to buy their drugs. If you watch TV or read any mainstream magazines, you cannot help but become inundated with ads for drugs to cure any problem you can think of.
There are many other egregious practices that go on in Big Pharma and which are beyond the scope of this blog. My point in writing this was first to help alert you to the hypocrisy of the so-called drug wars and second to bring to your attention the inordinate amount of effort and money that Big Pharma spends in trying to get you to buy their drugs. If you watch TV or read any mainstream magazines, you cannot help but become inundated with ads for drugs to cure any problem you can think of. The drug companies are the biggest pushers of drugs in the world today and all for a profit. The fact that these drugs may help your condition is very secondary to Big Pharma’s primary goal which is profits. The fact that many drugs should not be taken long-term and may have life threatening side effects is also not particularly important to the drug industry. Between the ignorance of many medical doctors anxious to provide a fast treatment and the greed of the drug industry, you had best become a very informed and cautious consumer of any drugs you are going to take. You should also be skeptical of any information provided by the drug industry.
The drug companies are the biggest pushers of drugs in the world today and all for a profit. The fact that these drugs may help your condition is very secondary to Big Pharma’s primary goal which is profits. The fact that many drugs should not be taken long-term and may have life threatening side effects is also not particularly important to the drug industry. Between the ignorance of many medical doctors anxious to provide a fast treatment and the greed of the drug industry, you had best become a very informed and cautious consumer of any drugs you are going to take. You should also be skeptical of any information provided by the drug industry.
 There is a difference between pain and hurt. When I tried to continue my ab exercises after my prostate surgery and then after my hernia surgery, I experienced pain. I wanted to get back into shape too quickly both times. I stopped the exercises and worked on other routines that did not cause pain. Mind you, the ab exercises still hurt and I have been doing them for six years. I am making a big distinction here between pain and hurt. Perhaps, I should say they “burn.” Burn is the athletic euphemism for hurt. Most people don’t like hurt. However, if you expect that you can get in shape without some discomfort, you are destined for life as a couch potato or in a surgery ward.
There is a difference between pain and hurt. When I tried to continue my ab exercises after my prostate surgery and then after my hernia surgery, I experienced pain. I wanted to get back into shape too quickly both times. I stopped the exercises and worked on other routines that did not cause pain. Mind you, the ab exercises still hurt and I have been doing them for six years. I am making a big distinction here between pain and hurt. Perhaps, I should say they “burn.” Burn is the athletic euphemism for hurt. Most people don’t like hurt. However, if you expect that you can get in shape without some discomfort, you are destined for life as a couch potato or in a surgery ward. Americans are enamored with diets and each new diet best seller promises fantastic results in a short amount of time. The Amazon number 1 best seller in the health and exercise category was a book titled “Big Fat Lies.” The author promises you the “truths” that helped her to lose 65 lbs. “without giving up pizza or ice cream.” The author is Kaelin Tuell Poulin and the book has a very high rating in the customer reviews section. Ninety-eight percent of the 235 reviewers gave it a 5-star rating. However, while I often put a great deal of store in ratings, you must be careful about inflated ratings. The one negative rater had this to say about the book: (typos in the review were not changed)
Americans are enamored with diets and each new diet best seller promises fantastic results in a short amount of time. The Amazon number 1 best seller in the health and exercise category was a book titled “Big Fat Lies.” The author promises you the “truths” that helped her to lose 65 lbs. “without giving up pizza or ice cream.” The author is Kaelin Tuell Poulin and the book has a very high rating in the customer reviews section. Ninety-eight percent of the 235 reviewers gave it a 5-star rating. However, while I often put a great deal of store in ratings, you must be careful about inflated ratings. The one negative rater had this to say about the book: (typos in the review were not changed)
 Two years ago, I started developing a pain in my right shoulder. I was not sure where it came from but after several months of it getting worse, I went to see an orthopedic doctor. He asked what if anything I might be doing to aggravate the shoulder. I mentioned that I swim frequently and am aggressive with my laps. His simple answer was “Well then, stop swimming.” I decided to follow his advice and for the next year, I stopped swimming. However, my shoulder pain did not get any better.
Two years ago, I started developing a pain in my right shoulder. I was not sure where it came from but after several months of it getting worse, I went to see an orthopedic doctor. He asked what if anything I might be doing to aggravate the shoulder. I mentioned that I swim frequently and am aggressive with my laps. His simple answer was “Well then, stop swimming.” I decided to follow his advice and for the next year, I stopped swimming. However, my shoulder pain did not get any better. Some people are not so lucky. However, I hesitate to call all of my good health “Luck.” There is a saying by Thomas Jefferson that “The harder I work the luckier I get.” I have worked hard to stay in shape. I exercise regularly. I watch what I eat. I try to avoid excesses. No doubt, I have had some luck that goes beyond hard work and discipline. Nevertheless, I believe that hard work and discipline has played a large role in my ability to be healthy and still active at my age.
Some people are not so lucky. However, I hesitate to call all of my good health “Luck.” There is a saying by Thomas Jefferson that “The harder I work the luckier I get.” I have worked hard to stay in shape. I exercise regularly. I watch what I eat. I try to avoid excesses. No doubt, I have had some luck that goes beyond hard work and discipline. Nevertheless, I believe that hard work and discipline has played a large role in my ability to be healthy and still active at my age.

 If homo sapiens have a weak link in their skeletal structure it is the back. It has been argued that the problem arose when we switched from hanging in trees to walking upright. Whatever the cause, back problems are easily the most common and perhaps one of the most painful problems faced by Americans today. I have heard it said that the “opioid epidemic” is really a “pain epidemic” as more people age and have to deal with back problems, knee problems and hip problems. No one beset by continuous pain can be blamed for wanting to find an escape from that pain. However, as I noted in the previous blog, this desire to escape pain often leads to bad choices. Surgery is too often prescribed when other treatment modalities would be more effective with less side effects. This brings us to the issue of chiropractic adjustments for back pain. How effective are they? Here is another comment from Dr. Preston H. Long regarding the effectiveness of spinal manipulation:
If homo sapiens have a weak link in their skeletal structure it is the back. It has been argued that the problem arose when we switched from hanging in trees to walking upright. Whatever the cause, back problems are easily the most common and perhaps one of the most painful problems faced by Americans today. I have heard it said that the “opioid epidemic” is really a “pain epidemic” as more people age and have to deal with back problems, knee problems and hip problems. No one beset by continuous pain can be blamed for wanting to find an escape from that pain. However, as I noted in the previous blog, this desire to escape pain often leads to bad choices. Surgery is too often prescribed when other treatment modalities would be more effective with less side effects. This brings us to the issue of chiropractic adjustments for back pain. How effective are they? Here is another comment from Dr. Preston H. Long regarding the effectiveness of spinal manipulation:

 My disclaimer is that this does not make me an expert. In fact, I would maintain that expertise in medicine is like the five blind men who were trying to describe an elephant. Each man had a different perspective on what an elephant looked like. Individually, no one perspective was a very adequate description of an elephant. It would take a synthesis of all perspectives and even more to truly describe an elephant. That is the problem with medicine. Too often, each professional looks at a problem through the narrow lens of their own discipline. The reality of a medical problem can often only be understood by multiple perspectives because of the interaction of the systems that make up the human body. This defining perspective of the problem seldom occurs both because of the nature of medical practice and many times because of the egotism of the so-called medical experts we consult.
My disclaimer is that this does not make me an expert. In fact, I would maintain that expertise in medicine is like the five blind men who were trying to describe an elephant. Each man had a different perspective on what an elephant looked like. Individually, no one perspective was a very adequate description of an elephant. It would take a synthesis of all perspectives and even more to truly describe an elephant. That is the problem with medicine. Too often, each professional looks at a problem through the narrow lens of their own discipline. The reality of a medical problem can often only be understood by multiple perspectives because of the interaction of the systems that make up the human body. This defining perspective of the problem seldom occurs both because of the nature of medical practice and many times because of the egotism of the so-called medical experts we consult.

